How does OCD impact intimacy and relationships?

When most people think of obsessive-compulsive disorder (OCD), certain stereotypes might come to mind, like someone checking locks, excessively cleaning or lining up objects, “just right.” But these stereotypes don’t paint an accurate picture of the complexity of OCD and how it can manifest and impact the everyday lives of those experiencing it. For example, OCD can significantly impact sex and intimacy, and yet due to the very nature of OCD, these experiences are often hidden, misunderstood or avoided completely.
This article aims to change that by raising awareness, demystifying OCD, and helping you understand how it can affect sexual health and intimacy, specifically. If you’re wondering whether OCD is impacting your own life or someone you care about, are in a relationship or intimate with, we hope this piece will help you feel less alone, provide some understanding and highlight some of the steps you can take to begin to address it.
What is OCD?
OCD is a clinical disorder, which involves the presence of both obsessions and compulsions that significantly interfere with many areas of one’s life (including sex and relationships!). These obsessions and compulsions are often time-consuming, and can lead to significant anxiety and distress.
Obsessions are defined as recurrent and persistent thoughts, urges or images that are experienced as intrusive, unwanted, and that cause marked anxiety or distress.
Compulsions are defined as attempts to ignore, suppress or neutralise these thoughts, urges, or images with some thought or action (i.e., by performing a compulsion).
While we often associate OCD with visible compulsions—like washing hands repeatedly or checking locks, many people with OCD don’t show any outward behaviours at all. Instead, compulsions can take place mentally. This might look like replaying events, silently repeating phrases, or repeatedly checking thoughts, emotions and bodily sensations.
OCD is more common than you might think, with research from Swinburne University here in Australia indicating that 3% of Australians will experience OCD at some point in their lives. Despite being considered a prevalent disorder, OCD can feel incredibly isolating and shame-inducing for those who live with it.
The OCD Cycle
As humans, it’s normal and natural to experience intrusive thoughts - we’ve all had those moments when a random, seemingly strange thought unexpectedly pops into our heads (see: Common Intrusive thoughts). For someone experiencing OCD, significant meaning can be attached to these thoughts, and significant doubt, shame, anxiety and distress is often associated.
OCD can be thought of as operating in a cycle:
Intrusion: A random, unwanted thought, urge or image occurs, often related to a specific trigger/theme.
Obsession: Meaning is attached to the intrusive experience (e.g., “what if this means x?”).
Distress: Increase in anxiety and distress levels.
Compulsion: In an attempt to minimise or “get rid of” the anxiety, the person may then engage in a compulsion - whether it’s an outward behaviour (like checking, washing or tapping) or a mental one (like repeating affirmations, reviewing memories or checking body sensations).
Temporary relief: The compulsions may provide short-term, temporary relief for the person.
Long-term reinforcement: However, the cycle is then reinforced long term, and the intensity of the distress increases, as does the urge to perform compulsions in order to cope.
Here’s an example of what this might look like…
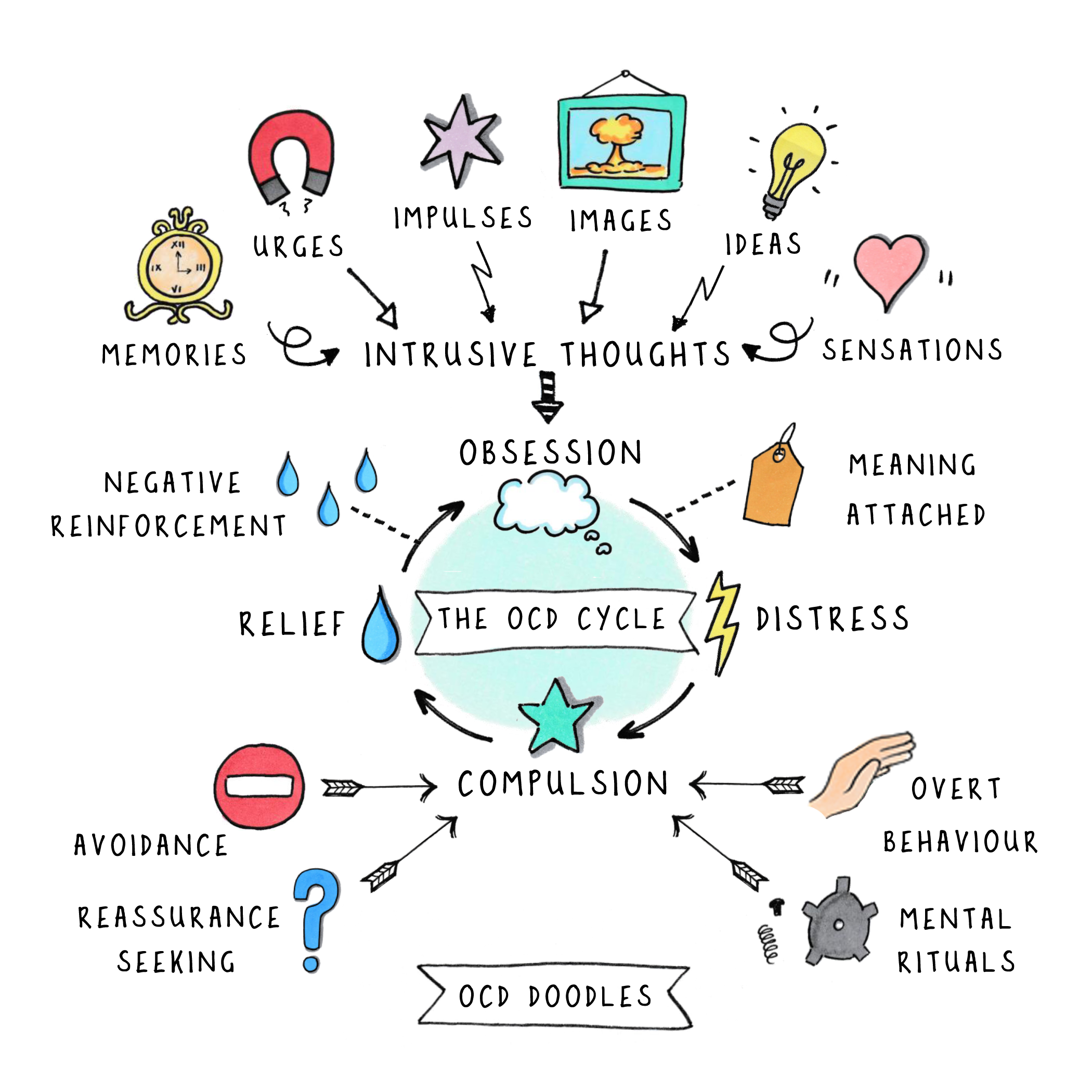
Illustration by OCD Doodle
Let’s say someone experiencing OCD has an unexpected intrusive image pop into their mind about hurting their partner in bed one night. They have no desire to hurt their partner, and the thought feels foreign, confronting and scary.
While some people might dismiss that thought as random, strange and unrealistic and leave it at that, for someone living with OCD, these intrusive thoughts may be considered particularly meaningful, they may think: “What if this means I’m going to hurt my partner?” “What if I’m dangerous?”
Understandably, panic and anxiety may follow, along with urgent attempts to suppress, disprove or get rid of the obsessive, distressing thought/s whenever they occur. This person might feel some immediate relief after they seek enough reassurance, mentally repeat affirmations about their nonviolent nature, or if they avoid bedtime with their partner completely to avoid the “risk” of harming them. However, over time, this reinforces the OCD cycle, and has the potential to limit that person’s life and relationships.
Often, the hardest part of living with OCD is that the intrusive and obsessive thoughts are often ego-dystonic, meaning they are in direct conflict with a person’s core values, beliefs, and identity - which is why they are so distressing! Unwanted thoughts can often attach themselves to what the person loves or values the most (e.g., their partner, their child, their health, their identity), so obsessing and attempting to suppress or get rid of these thoughts through whatever means necessary feels urgent and essential.
Unfortunately, suppressing these thoughts often makes them stronger, leading to a paradoxical situation where trying not to think about something makes it even more present and likely to show up. This is sometimes referred to as the “Pink Elephant Paradox” which describes how trying to suppress or avoid a thought makes it even more likely to stick around. Let’s try this out now, together…3-2-1 ....Do not think about a pink elephant…It’s incredibly important that you don’t have any thoughts about pink elephants right now!…How did you go?
What Are OCD Themes?
OCD often manifests in specific themes, which can help people understand how the disorder might show up in their lives. Some themes are more likely to affect relationships and intimacy. These include:
Relationship OCD: It's normal to experience doubts and reflect on the suitability of your relationships, but for someone with relationship OCD, they may spend excessive time and energy performing various compulsive behaviours in an attempt to gain complete certainty about their relationships. This can affect not only romantic or intimate relationships but also friendships and family connections.
Sexual Orientation OCD: While it is healthy and normal to explore your sexuality, someone with OCD may get stuck in obsessive thoughts about their sexual identity. They might spend excessive time obsessing about and doubting their sexual orientation and whether their feelings are "right." They might spend much of their time engaging in various compulsions to try to have complete certainty around any doubts related to their sexual orientation.
Contamination OCD: It is natural to want to avoid becoming unwell, but for someone experiencing OCD, they often feel distress, discomfort, or a sense of uncleanliness when they touch things they perceive as contaminants (such as substances, objects, people, etc.). In these cases, the concern about contamination is often out of proportion to the actual likelihood of harm.
Scrupulosity OCD: Scrupulous OCD involves obsessions related to religion and/or morality. Individuals with this condition may become overly concerned that something they thought, felt, or did could be a moral or religious transgression. This leads them to be consumed by worries about what their thoughts or actions say about their character and the kind of person they are. You do not have to be religious to experience this theme.
Paedophilia OCD: This theme involves intrusive, unwanted thoughts that are harmful or sexual, concerning children specifically. It’s crucial to emphasise and differentiate this OCD theme from paedophilic disorder; the significant difference being a lack of desire, arousal or urges associated with these thoughts. Instead, intrusions are often extremely distressing for the person, with feelings like disgust, shame, panic, and guilt.
How OCD Can Impact Intimacy
Sex and intimacy can be particularly difficult for those living with OCD because of how themes (like the ones discussed above) can be triggered in sexual and intimate contexts. Here are some examples of what obsessive thoughts might look like in intimate contexts:
“What if a bad thought pops into my head during sex? Does that mean I like the thought? Does it make it more real?”
“What if I don’t want to have sex with my partner right now? Does that mean I’m not in love with them and lying to them?”
“What if I catch an STI? Or what if I already have an STI and don’t realise it and will pass it on to someone else? I’ve used protection, what if it’s still not enough?”
Compulsions to try and get rid of these worries and fears might look like:
Mental rituals: Checking body sensations, repeating affirmations, or engaging in silent prayer.
Overt behaviours: Engaging in safety behaviours or rituals like excessive cleaning or using excessive forms of protection.
Reassurance-seeking: Asking partners for reassurance or confessing intrusive and obsessive thoughts.
Avoidance: Avoiding certain loved ones, sexual acts, or intimacy altogether.
Impact on Sexual Responses
OCD can also interfere with sexual functioning. Research has shown that OCD symptoms are associated with higher rates of sexual issues and lower sexual satisfaction. The sexual response cycle can include experience of: desire, arousal, orgasm, and resolution (but not necessarily all or one after the other). Let’s look at some examples of how obsessions and compulsions might impact each one:
Desire: Desire describes a person's interest in sexual activity. If you experience OCD your desire for sex may be impacted, as intimacy could be a significant trigger for distressing thoughts about your relationship, your identity, your potential to experience or cause harm.
Arousal: Arousal describes the neurological, physical, psychological response to sexual desire. To experience arousal, your body requires conditions of safety and excitement. If your body is in a state of fight/flight/freeze due to distressing thoughts, urges and/or images, your sympathetic nervous system may disrupt your ability to effectively experience arousal.
Orgasm: Orgasm is an experience of peak sexual pleasure, in response to accumulated sexual excitement, often including muscle contractions and hormonal releases. If you live with OCD your ability to remain present and embodied during sex may be disrupted by intrusive and obsessive thoughts and/or compulsions; this may interrupt the natural accumulation of excitement that could have otherwise occurred.
Resolution: Resolution occurs after you have experienced peak sexual pleasure, when the body returns to a naturally relaxed state. For someone with OCD, this phase might be interrupted by residual feelings of distress, shame, or disgust, especially if ego-dystonic thoughts were experienced during sexual activity.
An important note: while we are exploring each of the four stages of sexual response and how OCD can influence them, it's crucial to remember that our sexual responses are uniquely personal and can vary greatly from one person to another. So, while it can be helpful to consider how OCD might be affecting your sexual experiences, it's also just as important to recognise that fluctuations and differences in your sexual responses are entirely normal! Whether or not OCD is part of the picture, it's natural for these stages to ebb and flow over time, or for you to not experience a particular stage at all. Everyone’s experience with intimacy is different, and these shifts are a part of what makes each person’s sex and intimacy journey so individual.
What You Can Do
Remember, you are not alone.
Living with OCD can feel shameful and isolating, but it's important to remember that you're not alone. Intrusive thoughts are a natural and normal part of being human (see: Common Intrusive thoughts); and even the desire to avoid, suppress and minimise suffering is a shared human experience, too!
One approach that can be helpful in responding to shame can be practicing self-compassion (shame’s arch nemesis!). Where shame encourages us to feel inferior, isolated and to hide these experiences away, self-compassion reminds us that suffering is a part of the shared human experience, and not something that happens to you, alone.
Remember, you are not your thoughts.
Intrusive and obsessive thoughts can feel all-encompassing, but they don’t define you. Thoughts are not “good” or “bad,” they just are; they also are not a reflection of your worth, values, ethics or behaviour.
If you feel this way, you may be falling into the thought-action fusion trap, where you believe just thinking about an action morally equates with actually taking that action and/or increases the likelihood of you taking the action. However, the ultimate irony is, the very distress these thoughts are causing you is a clear sign that you are very strongly opposed to them!
One approach that can be helpful is to create some distance between yourself and your thoughts by using “defusion” strategies; they can help by changing our relationship to your thoughts by observing them, rather than engaging with them or taking them too seriously. You can do this by first noticing you’re having the thought and then applying a strategy that creates space between your observing self and the thought, like: “I’m having the thought that x.” You can sing the thought to a funny tune, give the thought a character’s voice you wouldn’t take seriously, or respond with “thank you, mind!” By practising these defusion skills regularly, eventually, you can begin to develop an understanding that thoughts are merely that – thoughts!
Remember, there is help.
Because OCD often latches onto what we care about or love most, those living with OCD often experience thoughts, images and urges that feel scary, shameful and taboo. This means that many people experiencing OCD may find it difficult to seek help or open up about their experiences with loved ones, or professionals. But, there is help available, and there are several therapies that have been found to be effective in managing OCD. Some therapies shown to be effective for OCD specifically, include Exposure Response Prevention (ERP); Acceptance and Commitment Therapy (ACT); Eye Movement Desensitisation Reprocessing (EMDR); and Relationships Therapy. It might also be helpful when looking for a therapist, to ask if they have experience and training in working with OCD specifically to ensure they have a thorough understanding of what you might be experiencing.
Conclusion
Sexual health, intimacy and relationships are incredibly important foundations for our wellbeing as human beings, and while living with OCD may make discussing these topics more challenging, I hope this article has shed light on what may be happening for you or someone you know in more depth, and increases awareness and ultimate understanding for those living with OCD. If this article has resonated personally, I encourage you to first and foremost know that you are not alone, there is nothing to be ashamed of and that you are worthy of care and compassion. Also, I hope this serves as a reminder of the importance of seeking support if you feel obsessions or compulsions might be getting in the way of you having the relationships and intimacy you desire and in leading a life that is most rich, full and meaningful for you.
Extra Resources
Website: https://www.intrusivethoughts.org/ Podcast: The OCD Stories
ARCVic Helpline: OCD & Anxiety HelpLine 03 9830 0533 or 1300 ANXIETY

AUTHOR
Sophie Capern
Psychologist
Related self-help courses and resources:
Understanding Arousal
Online course

Sexual Self Meditation
Online resource

Relationship Check-In Template
Online resource